The Iliopsoas Muscle and its Frequently Overlooked Syndrome
 The iliopsoas is comprised of two muscles: the iliacus and the psoas.
The iliopsoas is comprised of two muscles: the iliacus and the psoas.Introduction
Situated deep within our core, the iliopsoas muscle is one of the most complex structures in the body, playing crucial roles in hip flexion, postural stability, and walking.
However, its significance extends well beyond these roles, as it holds the key to unraveling a wide range of pain and dysfunction that cannot be detected through standard allopathic testing methods such as MRIs, X-rays, CT scans, or neurological tests.
Conditions like back, hip, groin, and abdominal pain often find their explanation in two notable conditions that can arise when the iliopsoas muscle becomes dysfunctional:
- Iliopsoas syndrome, a muscular condition...
- Pelvic torsion, a misalignment of the pelvic bones...
Both of these conditions are highly prevalent, yet they remain poorly understood within the realm of conventional medicine.
While our primary focus in this article will be on exploring Iliopsoas Syndrome, it is important to note that this syndrome often serves as a precursor for pelvic torsion. Therefore, when one condition is present, it is not uncommon for both to be present.
For a comprehensive discussion on pelvic torsion, refer to the complete article here.
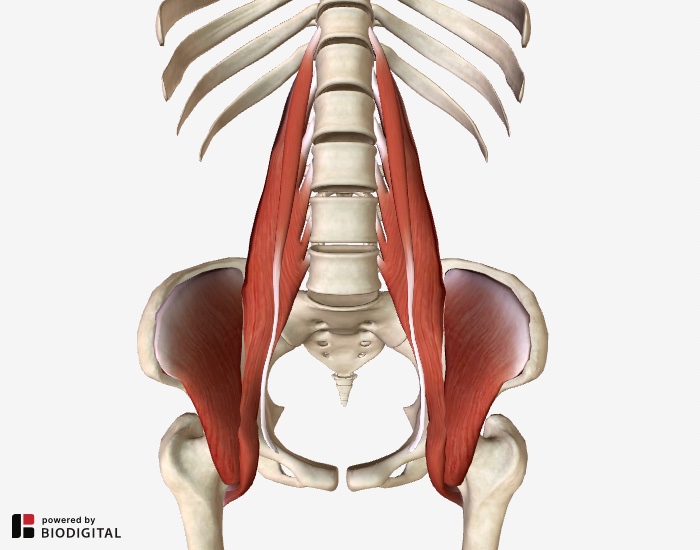
iliopsoas anatomy: two muscles in one
The iliopsoas muscle consists of two individual muscles - the iliacus and the psoas - which, despite their different origins, share a common attachment point.
The psoas major originates from the lumbar spine and intervertebral discs, descending obliquely to attach to the lesser trochanter, a part of the upper inner thigh bone (femur).
Originating in the upper two-thirds of the iliac fossa, the iliacus merges with the psoas major tendon, with some of its fibers directly connecting to the lesser trochanter.
The primary function of the iliopsoas is hip flexion, responsible for lifting the leg during walking and other activities.
Due to its attachment along the lumbar spine, the psoas also plays a crucial role in maintaining upright posture and can assist in extending the lumbar spine in coordination with the back muscles.
Prolonged periods of sitting, such as during driving or desk work, can lead to shortening and tightening of the iliopsoas, especially if regular stretching is neglected.
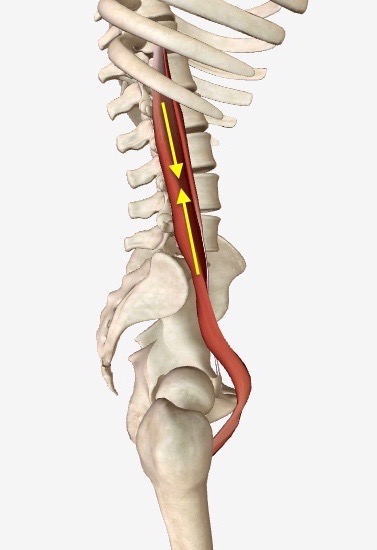 Right side view of psoas muscle. Hypercontraction can reduce natural lumbar lordosis.
Right side view of psoas muscle. Hypercontraction can reduce natural lumbar lordosis.the diaphragm muscle, the PSOAS muscle and breathing
One of the least-discussed topics in the literature is the relationship between the diaphragm muscle, which controls breathing, and psoas muscle which is positioned just below it.
The diaphragm is what pulls air into, and expels air out of, the lungs. Here is its action. The animation is interactive. You can zoom in, spin the model around, etc.
If we consider the diaphragm and the psoas together we can begin to get a sense of the importance of their relationship. Here the diaphragm and the psoas muscle are shown together.
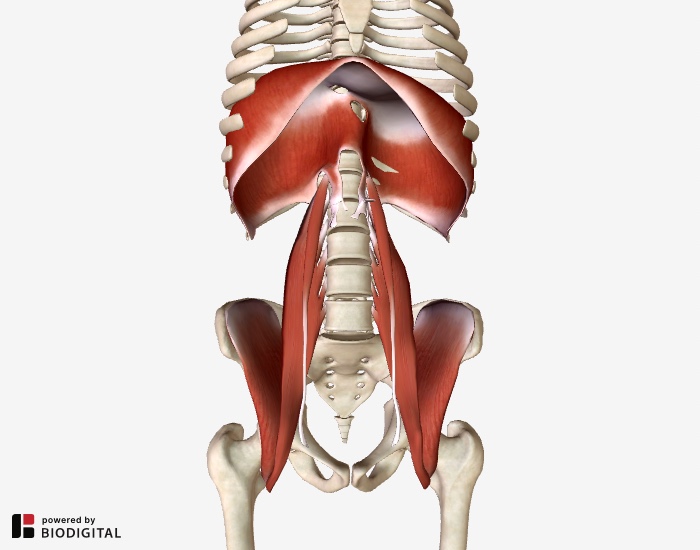 Diaphragm and iliopsoas
Diaphragm and iliopsoasIf we look closely, we can see the actual interweaving of the two muscles at T12 through L2.
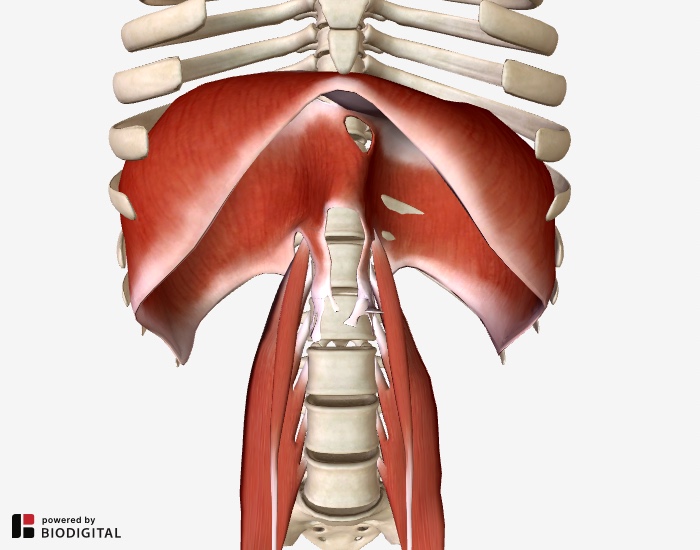 Diaphragm and psoas muscles. Close front view.
Diaphragm and psoas muscles. Close front view.What's most unique about the diaphragm muscle and the psoas muscle, however, is their physical position and orientation to the abdominal viscera.
As you can see below, all of our digestive organs are packed into the space just below the diaphragm.
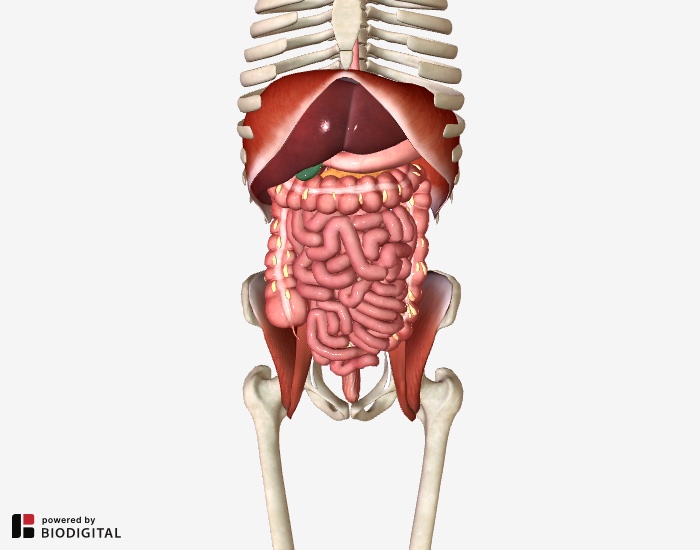 Digestive organs packed in below the diaphragm and on top of the psoas.,
Digestive organs packed in below the diaphragm and on top of the psoas.,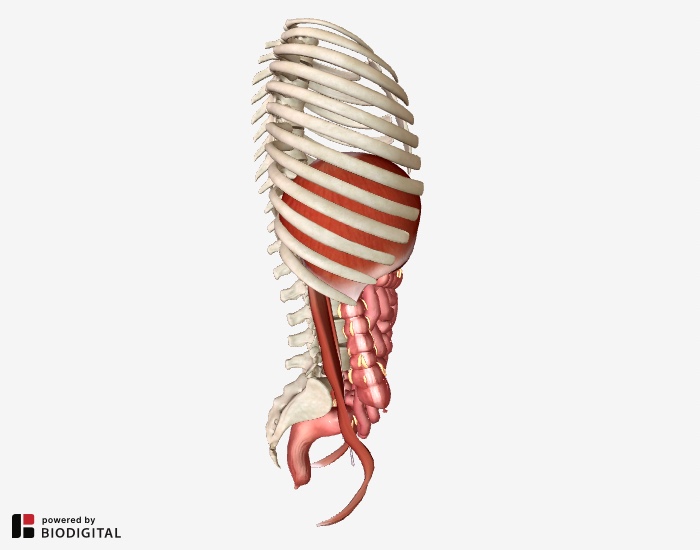 Digestive organs packed in below the diaphragm and in front of the psoas. Side view.
Digestive organs packed in below the diaphragm and in front of the psoas. Side view.All these organs are contained within a sac called the peritoneum. Imagine this sac as being like a big water balloon.
In normal, healthy, relaxed breathing, the diaphragm flexes down on this water balloon causing it to flex and bulge. With every breath, this bulging and reshaping acts as a kind of massage for the psoas.
The normal respiratory rate for an adult is 12 to 20 breaths per minute. That calculates to 720 to 1200 breaths per hour or 17,280 to 28,800 breaths in a 24 hour period.
That's an extraordinary opportunity for the action of breathing to be exerting a positive impact on the psoas.
When our breathing is shallow or paradoxical, on the other hand, the diaphragm does not flex down fully in this beneficial manner.
In shallow or paradoxical breathing, the abdominal muscles can remain clenched causing two unwanted effects:
- Abdominal clenching -- that is, the abdominal muscles held in a persistently contracted state -- reduces the space and capacity for the diaphragm to flex downward, thus disabling a full breath, and severely limiting the beneficial downward pressure on the water balloon-like peritoneum.
- Abdominal clenching reduces flood flow to the region. Like a clenched fist in which the knuckle goes white, persistently contracted abdominal muscles push a healthy blood flow out of the abdominal region setting the stage for the iliopsoas to become ischemic.
Ischemia, then, sets the stage for Iliopsoas Syndrome.
Iliopsoas Syndrome
When the psoas muscle or iliacus muscle becomes ischemic it can be the source of a bewildering variety of mysterious and hard-to-diagnose pain.
In Myofascial Pain and Dysfunction: The Trigger Point Manual, by Janet Travell M.D. (personal physician to President John F. Kennedy) and David Simons, M.D., this muscle is referred to as "the hidden prankster.”
These two eminent and long-time pain researchers could hardly have come up with a more fitting label for this muscle.
In my clinical experience I have found that dysfunction of the iliopsoas — commonly referred to as Iliopsoas Syndrome — is responsible for more unexplained back, hip and leg pain than any other single cause.
Potential regions of pain
Over the course of thirty years in clinical practice treating iliopsoas dysfunction, clients have presented with pain in following areas...
|
The problem an individual may face when being examined by a physician not trained in muscular problems is that examination of any of the above areas of pain may reveal exactly nothing.
Many standardized allopathic tests, including neurological tests, will come back normal because they are not tests designed to evaluate muscular problems. Such problems can only be properly assessed with skilled palpation and knowledge of musculoskeletal dysfunction.
Of particular difficulty in the case of the iliacus is the fact of its hidden location. This muscle is not easy to palpate if you don’t have any practice at it. The psoas is more accessible but no less intimidating to palpate, much less treat, if you’re unsure of what to do.
causes of Iliopsoas Syndrome
A very common problem for the iliacus and psoas is that they both can shorten over time, especially in those individuals who sit for long periods of time.
Prolonged sitting in which muscles are in a shortened state for extended periods can lead to the muscles adapting to this position.
Once in an adapted state, muscles have trouble returning to their normal resting length. This is a basic characteristic of muscle function.
The Cross-Bridge Theory, which attempts to explain the contractile action of muscle tissue, asserts that, once contracted, a muscle cannot lengthen on its own.
The contractile units of the muscle (sarcomeres) must be stretched back to their original resting length by an outside force (such as an opposing muscle group) before the muscle is able to actively contract and relax again.
Can you just stretch the muscle out then?
Yes... if the proper type of stretching is done. For example, I have found the method of Active Isolated Stretching to be vastly superior to static stretching, especially in cases where muscles are stubbornly tight.
In some cases the stretching is enhanced by manual therapy because muscle fibers can become adhered or stuck together.
Sometimes this "adhering" is within the muscle itself. Other times the compartment of one muscle can become adhered to the compartment of another muscle.
In both cases the attempt of the muscle to fully lengthen or fully contract is impeded. This results in a dysfunctional muscle which can be painful in and of itself, but also can result in compensatory muscle patterns throughout the body.
This is one reason, for example, a dysfunctional iliopsoas muscle on the right side of the body could result in pain on the left side of the body. One side of the body might be fixed in place while the other side might be strained from overuse.
consequences of chronic muscular contraction
If a muscle cannot return to its normal resting length, it then resides in a state of chronic contraction and numerous undesirable consequences can result:
1. Ischemia
A chronically contracted muscle can become ischemic (low blood flow). Imagine the white knuckles of a clenched fist. No blood flow there. An ischemic muscle is often a painful muscle.
2. Trigger Points
A chronically contracted muscle can develop trigger points which refer pain (or numerous other possible sensations – thermal, tingling, numbness, aching) either radiating out from the muscle or felt in other parts of the body.
3. Distorted Movement Patterns
A chronically contracted muscle can distort the movement of the joint it crosses. For example, a chronically tight iliacus could reduce movement at the front of the hip.
4. Muscular Compensation
A chronically contracted muscle can cause other compensations or distortions in the body. If a chronically tight iliacus, for example, reduces movement in one hip, then the other hip or the spine or other parts of the body will be called upon to compensate or to change their normal pattern of movement.
5. Nerve Entrapment
A chronically contracted muscle may be responsible for entrapment of nerves, another cause of pain. In the case of the iliopsoas, entrapment of the following nerves is possible: the femoral nerve, the lateral femoral cutaneous nerve, the femoral branch of the genitofemoral nerves, the iliohypogastric nerve and the ilioinguinal nerve.
Iliopsoas Syndrome & Pelvic Torsion
When the iliopsoas muscle experiences ischemia, both the iliacus and psoas muscles can suffer from dysfunction, as discussed previously.
However, one specific way in which the iliopsoas can become dysfunctional is through an asymmetrical shortening of the hip flexors, resulting in pelvic torsion.
Pelvic torsion occurs when the iliacus muscle on one side and the psoas muscle on the other side both become locked in a shortened state.
The tight and shortened iliacus on one side causes the pelvis to rotate forward, while the tight and shortened psoas on the other side holds the pelvis fixed in place.
As a consequence, the pelvis becomes misaligned, altering the level of the hip joints and leading to a functional leg length discrepancy. This chain reaction triggers muscular compensation throughout the body, potentially resulting in various discomforts and dysfunctions.
For a comprehensive understanding of pelvic torsion, refer to the detailed article available here.
It is important to note that the conditions giving rise to Iliopsoas Syndrome are the same conditions that contribute to pelvic torsion. Consequently, these two conditions often manifest concurrently.
To address these issues, I have developed comprehensive self-guided video courses that can be followed in the comfort of your own home.
These course options are described below in the What To Do section.
How to resolve Iliopsoas Syndrome & Pelvic Torsion
Years ago, I was receiving a lot of inquiries from all over the world about an earlier version of this article about Iliopsoas Syndrome.
Those writing in believed that they were suffering from this condition and were desperate for help.
While a few were able to visit my clinic in Vermont, that was impossible for most.
So I began to develop protocols that anyone could do at home, protocols that would mimic how I helped individuals to relieve Iliopsoas Syndrome.
Those protocols became the self-guided course, "Healing the Hidden Root of Pain: Self-Treatment for Iliopsoas Syndrome."
The 2013 Course for Resolving Iliopsoas Syndrome
In 2013, I launched a self-guided online course dedicated to resolving Iliopsoas Syndrome: "Healing the Hidden Root of Pain: Self-Treatment for Iliopsoas Syndrome."
This course presents a comprehensive 4-Phase process designed to address the underlying causes of the syndrome. It includes various methods and techniques, such as self-massage, proper breathing, Somatic Movement, stretching, and strengthening exercises, specifically tailored to enhance iliopsoas function and provide long-term resolution.
While this course is still available for purchase, please continue reading below to discover how you can receive this course for FREE.
The 2022 Course for Correcting Pelvic Torsion
What’s not included in the 2013 course is instruction for resolving pelvic torsion, despite the fact that these two conditions are closely related.
Back then, I had not yet developed an easily accessible protocol that the general public could use for correcting pelvic imbalance.
Because pelvic torsion can be confusing (even to health practitioners) and because great care must be applied when applying corrective techniques to remedy pelvic torsion, I felt a separate course was needed.
Nearly ten years later, that course became a reality.
In 2022, I introduced the "Postural Blueprint for Correcting Pelvic Torsion: The Complete Guide to Restoring Pelvic Balance."
This course incorporates six distinct exercise groups, including:
- Somatic Movement
- Pelvic Counter Rotation
- Active Isolated Stretching
- Improving Squatting Competence
- Core Strengthening
- Back Line Strengthening
The Postural Blueprint for Correcting Pelvic Torsion is the only course of its kind available anywhere, providing a comprehensive solution for addressing the widespread and persistent problem of pelvic torsion.
Better Together
Given the close relationship between Iliopsoas Syndrome and Pelvic Torsion, I wanted to ensure that as many people as possible have access to both courses.
Because these two courses work synergistically, I have bundled them together...
Released a decade apart, these two courses offer the most comprehensive self-treatment available anywhere, allowing you to resolve Iliopsoas Syndrome and correct pelvic torsion effectively.
While many individuals have successfully resolved Iliopsoas Syndrome with the guidance of "Healing the Hidden Root of Pain" alone over the past ten years, the "Postural Blueprint" specifically addresses the challenging condition often associated with Iliopsoas Syndrome: pelvic torsion.
Return to Top | Causes Index | Home Page
Anatomy Images Courtesy of BIODIGITAL
The Iliopsoas Syndrome ForumTHE FORUM IS CLOSED TO NEW SUBMISSIONS BUT YOU'RE WELCOME TO EXPLORE TO DETERMINE IF THIS IS THE PROBLEM YOU'RE STRUGGLING WITH. |
What Other Visitors Have Said
Click below to see contributions from other visitors to this page...
Jane moxey 
I think this could be me! Have a strange whirring sensation inside left groin..not painful but often causes the left leg to have problems in going forward …
Questions about my pain
I developed on and off groin pain about a year ago. I started hurting in my pelvic area. June 2015, I had a CT scan without dye and it showed a bladder …
Groin and Hip Flexor Pain
Hi
I had bilateral hip arthoscopies last year. My right hip was done in May 2014 and then the left in July 2014.
My hip pain actually began in November …
24/7 Chronic Pain
Following more than a decade of sport related pain (so I thought), I was diagnosed with Spondylolithesis S1/L5 and had a spinal fusion in 1998.
Since …
Injured Police Officer
I have spent much of my adult with some low back pain, but never so much that it was more than a troubling annoyance. Chiropractors told me I had tight …
Longtime Runner Trying to Self-Diagnose
I have been running for close to 20 years, and my body is finally starting to break down from it's dysfunction and lack of strength and mobility in my …
Pain Came Back with a Vengeance
I am a 34 year female, I was pretty active prior to my injury. I was involved in a motor vehicle accident almost 14 months ago.
I was at a complete …
My Self-Diagnosis of Iliopsoas Symptoms
I sit for 4-6 hours daily. I get my exercise by walking, gardening, housework and outdoors activities (swimming, sailing, kayaking and hiking). I believe …
Pelvic Pain of Unknown Origin
I am a 30 year old female. Former runner and soccer player and what you would describe as the 'jock' type: always active, strong, and in shape. I’ve never …
Trochanteric Bursitis and Iliopsoas Syndrome
The pain started early in January 2012, but being a stalwart runner, I thought a couple of weeks off and it would go away. Wrong.
While I waited for …
3 Years of Recurring Hip Pain
I never knew what happened to make my hip begin to hurt. I am a runner. I was running 4-5 miles per day with longer runs on the weekend. My hip started …
From Fit and Happy to Disabled and Depressed
My story is very similar to the others here. I was in terrific shape, teaching 2 fitness classes a day. I had energy to be active in all areas of my …
Is the Psoas Muscle Causing My Husband to Bend Forward?
My husband is 67 and has had every test imaginable (11 different Doctors and Chiropractors) and nothing has manifested. He walks bent over sometimes almost …
Seven years of pain - is it the psoas?
My daughter has suffered right lower quadrant pain for 7 years. It started when she was ten. She has had every test you can think of. Doctors thought …
Pain at Top Corner of Pelvis, Hip Flexors, and Lower Back
Pain in my hip area began about 8 weeks ago. I'm a runner, so I stopped running, as the pain was getting progressively worse. I took it to be a standard …
Desk Stretches Helped
My problem started after high kicks. Most probably it happened because I started on a cold body and straight away began kicking with high intensity. …
Dull Pain in My Groin
I'm a sheriff's deputy and sit in a patrol car for sometimes hours at a time. I began experiencing dull pain in my groin, a pulling/aching sensation behind …
Pain in My Lower Back
I am not sure if this is what I have but it sounds a bit like it, in that as time has gone on, it has developed from one set of nerve pain to involve different …
Running Out of Non-Surgical Options
I am a low back (L5-S1) patient that has had everything done over the past four years without any success (only local 3-4 level pain when walking that …
So I'm not crazy?
I am a 28 year old female with no history of injury. I was a competitive cheerleader for four years but only suffered occasional leg pain during that time. …
Finally an Answer!!
I'm in my mid 50’s, female, very small & fit, active, quite strong. 25 years ago a chiropractor pulled on my right leg. I not only FELT it like a bullet, …
FRUSTRATED WITH MY DOCTORS...WONDERING IF I'M CRAZY
I have been suffering from low back pain on the right side for about 10 years now. I thought at first that it was just due to bad posture. I have always …
Multiple Diagnoses & Pain Before and After Hip Arthroscopy
In January of 2011, while at work, I experienced a shooting pain in my left buttock (which I did not understand at the time was really part of my hip). …
Terrible Time Walking
My present age is 57 and I am female and slim. About 7 yrs. ago, I was beginning to learn the banjo. I sat a lot holding this 17 lb. instrument while practicing …
My Doctor Thinks I'm Crazy
I have suffered from both low back pain and pain between my shoulder blades for years. It all started when I was pregnant with my daughter about 4 years …
Diagnosed with Psoas Syndrome
Back in September 2010 I jumped down from the back of a truck and injured my thigh. I did not realize it was serious until I could not stretch or do exercises …
Hidden Prankster Sufferer
I think that I have this "hidden prankster" syndrome. I have suffered back pain for many many years.
I have tried Pilates but some of the exercises …
Cramping in Upper Thighs
I have been riding a stationary bike for over a year for a minimum of 45 minutes a day followed by sit-ups.
I started to have extreme cramping in my …
My Iliopsoas Dysfunction Discovery and Yoga
I'm a 56 year old female. I have had chronic back pain for over a decade. I have been to many doctors and every time they found nothing. I had the usual …
Pain After Cycling
4 years ago I returned from a 10 day sea kayaking trip and went straight on a cycle tour in mountainous terrain.
I bent over to pick up a friend's punctured …
Finally the Answer to My Dilemma
Ten months ago I suffered a lower back injury while bending repetitively. After approximately ten sessions of physiotherapy and rest and gentle regular …
Disabled and suffering
I am a student and also suffer from a seizure disorder and fainting spells which prevent me from exercising and stretching on a regular basis. From everything …
Bike Accident
Fell off my bike in summer 2009 right onto my greater trochanter. I was traveling at speed and hip took full force because my shoes were clipped in. I …
Injured International Hockey Player
I was an extremely fit international hockey player and one day I finished a game and was very stiff. My back had seized up and I could hardly walk. I got …
20 Months of Pain Getting Worse
I think it may have started at the gym when I overdid an exercise on a hip-flexing machine. I had a pain in my groin and down the inside of my right leg …
Injured Professional Surfer
I am a professional surfer from France and I have been injured for a total of 29 months since I pulled something during a surfing session. Since that day …
10 Year History of Pelvic, Groin, and Low Back Pain
I m a 40 year old female and have had chronic left sided groin, low back, hip, and pelvic pain for about the past 10 years.
I have tried many different …
Tired of the pain. Not rated yet
Pain started one night in right lower back and radiated to the side. I was unable to pin point the exact location of the pain but felt it was just inside …
Possible Iliopsoas syndrome? Don't know Not rated yet
I'm now 5 1/2 weeks dealing with this pain out of nowhere. It hit me initially in right glute and nearly buckled me to the ground. The intensity was a …
Grandmother in pain Not rated yet
My pain is in my right lower back, buttock, groin and pelvic floor.
It sometimes gives me tight calf muscles. I have been seeing an osteopath and chiropractor …
Retired CNMT Not rated yet
I am a 73-year old female and have been retired as a CNMT for ten years. About three years ago at an outside training session with my Labrador Retriever, …
A Crash to the Ground Not rated yet
Hello. I fell from a height of 2 ft. smack down on cement with my legs stretched out on Nov. 2. I was babysitting my 2 1/2 year old granddaughter and …
Standing too long! Not rated yet
I had been wearing my beloved toe shoes for three years and standing on concrete floors too many hours. I developed a deep pain in the fold between leg …
Labral Tear with Iliopsoas Syndrome Not rated yet
I suffered an anterior labral tear to my hip three years ago. I cannot take anti-inflammatory meds but swim and bike as much as I can.
Recently, my …
Congenital Hip Malformation Not rated yet
Unbeknowst to me, I was born with a congenital hip malformation.
One side of my hip had no hip socket. The femoral ball attached itself to the hip …
Sudden Pain Out of Nowhere Not rated yet
I had just walked into my home when out of nowhere a very sharp pain hit me in my hip. I was not sure what had just happened. All I knew is that I had …
Pilates Trainer with Chronic Hip Pain Not rated yet
Hello. I'm 42, female and had fusion surgery 11 years ago in my lumbar region. I had a quick recovery, got into fitness training a year after my surgery, …
Father of Triplets Can't Stand Up Not rated yet
I first noticed this pain in my mid-twenties while playing in a flag football league, but it was not as debilitating as it is now.
Now I’m 36 and one …
Runner with Hip and Lower Back Ache Not rated yet
I've been struggling with an aching pain in my hip for some time while training for a marathon.
The pain doesn't inhibit my ability to run but certainly …
Belly Dancer with Back Pain Told to Strengthen Abs Not rated yet
My first memory of back pain was when I was in my mid- teens. I was in a play and one scene was rehearsed again and again forcing me to stand for a couple …
My Sister Injured While Skiiing Not rated yet
My sister fell while skiing in early December. She believed she injured her knee and the emergency room physician placed her in a universal splint and …
Camel Pose and Table Pose Relieve Pain Not rated yet
From time to time I get the sensation of a slightly pulled muscle. This develops by the next day into a very severe pain which shoots from my lower left …
Suffered for 5 Years Not rated yet
My name is Jan and I've suffered for at least 5 years with psoas pain. It started when I had knee pain and went to an orthopedic surgeon.
The MRI didn’t …
I Thought it Was Sciatic Pain Not rated yet
The sharp pain in my sacral area started a few years ago. I get tingly feet and my legs feel fatigued as if I’ve just run a marathon.
When I stretch …
Lower Back, Lower Abdomen, Aching Legs Not rated yet
I have had several bouts of lower back pain in my life. I'm now 48. I work a physical job so think nothing of it. Yes, it's my back.
But I had a hysterectomy …
Back Pain During Pregnancy Not rated yet
I've suffered with lower back pain for the past five years. After MRIs, CT scans, X-rays, Neurologists etc, I was diagnosed with fibromyalgia and sciatica. …
Extreme Lower Back Pain Not rated yet
After spending a month in the hospital and two months resting at home after having abdominal surgery, my lower back felt as if I had been hit by a 4 x …
Work injury Not rated yet
In April of this year I was injured in an explosion at my job. A piece of metal punctured my abdomen at high velocity like a gun shot. The projectile lodged …
This page has "me" written all over it! Not rated yet
I'm going to try to be as brief as possible!
I'm an 18-year-old female that's has chronic, severe tendonitis in my iliopsoas tendon for over 4 years. …
Groin Pain Not rated yet
I have suffered with groin pain for about 3 years. I had cortisone shots in my hip and groin area 2 years ago. When it didn't work they gave me another …
Terrible Hip pain! Not rated yet
During my 22 years in the Army I always had some back problem but nothing I could not stretch out and continue exercising and have normal movement.
…
Condition arose during pregnancy! Not rated yet
I'm 7 months into my first pregnancy and I am in absolutely excellent health. I have not gained much weight and am just starting to show a belly.
For …
TIGHT ILIACUS Not rated yet
My physiotherapist diagnosed a tight iliacus and psoas last January. After only one massage treatment the psoas loosened up but it's been 4 months and …
Feeling Much Better Not rated yet
Dear Stephen O'Dwyer,
I can not find words to tell you how grateful I am! You literally saved my life from every day and every night pain.
It all …
Dangerous Condition? Not rated yet
Sounds like me, I have the symptoms almost to the core of what you say can present. Dr. hasn't figured it out yet. Haven't had MRI yet but hoping for …
Distance Runner Hip Pain Not rated yet
I am a collegiate distance runner who has been out for 4.5 months. From December 20th to March 7th I was recovering from bilateral femoral stress fractures. …
Hip and groin pain Not rated yet
I am a 55 year old woman. About 10 years ago I began having pain deep on my hip in the middle of the night. Sometimes it was my left hip, other times my …
Long Distance Driving Causing Pain Not rated yet
I am a 54 mother of three teenage children. I am 5'2" tall and weigh about 8 stone (128 lbs I think). Until the children started at secondary school …
Pain and Weakness in My Right Leg Not rated yet
I'm not exactly sure how it happened, either by dead-lifting or by doing yoga.
It started out as a little bit of tightness in my hips and general …
Lower Back Pain for 4 Years Not rated yet
I got pregnant with my daughter 4 years ago and about 8 weeks later my lower back pain started. I was in pain my entire pregnancy, unable to enjoy any …
Goodluck to Me & My Iliopsoas Syndrome Not rated yet
I just read about this iliopsoas on your site and I think this is what I have. I've been suffering for 10 years now from this hip pain and every time I've …
"Hip Pain" Not rated yet
I'm an athlete who has been having this aching pain in my "hip" for almost a year now. Luckily it has not yet affected my performance because I don't usually …
Nerve Pain Might Be Iliopsoas Syndrome Not rated yet
I am an accountant so I sit for most of the day. I am very active but I have been limited over the last few years due to my hip problems. I had sciatica …
go to new course areaolder course area
|

|
CURRENT COURSES POSTURAL BLUEPRINT FOR CORRECTING PELVIC TORSION: The Complete Guide To Restoring Pelvic Balance (2022) STRETCHING BLUEPRINT FOR PAIN RELIEF & BETTER FLEXIBILITY: The Complete Guide to Pain-Free Muscles Using Active Isolated Stretching (2020) HEALING THE HIDDEN ROOT OF PAIN: Self-Treatment for Iliopsoas Syndrome (2013) FREE MINI COURSE: Introduction to Active Isolated Stretching |